Five newly discovered proteins patrol cell nuclei
▻https://massivesci.com/notes/five-new-nuclear-envelope-proteins-cells
These proteins might shed light on how to treat diseases like progeria
Five newly discovered proteins patrol cell nuclei
▻https://massivesci.com/notes/five-new-nuclear-envelope-proteins-cells
These proteins might shed light on how to treat diseases like progeria

Sanofi et Google renforcent leurs liens dans l’e-santé
▻http://www.lefigaro.fr/flash-eco/sanofi-et-google-renforcent-leurs-liens-dans-la-e-sante-20190618
Le premier groupe pharmaceutique français Sanofi et le géant mondial du numérique Google ont annoncé ce mardi une nouvelle collaboration sous la forme d’un laboratoire « virtuel » d’innovation, pour développer de futurs médicaments et services en tirant parti des technologies de données.
[…]
Sanofi compte notamment recourir à des techniques d’intelligence artificielle de Google afin d’établir « de meilleures projections des ventes » de ses traitements et répercuter ces enseignements sur ses activités commerciales et logistiques.
Sanofi drives digital transformation with Google Cloud
▻https://cloud.google.com/blog/topics/customers/sanofi-drives-digital-transformation-with-google-cloud
Sanofi and Google will work closely on two core initiatives. The first will be to build an Innovation Lab to test and explore solutions focused on how technology can:
– Enhance the understanding of patients and diseases
– Drive productivity gains for business operations
– Promote patient outcomes and access to healthcare through the use of technology
The Innovation Lab will bring together Sanofi executives and experts across Google to discuss challenges in the healthcare space and how we can create solutions together.
Secondly, Sanofi will leverage Google Cloud Platform to modernize their infrastructure, migrating workloads to the Google Cloud, and building an analytics and machine learning platform to glean better insights from their data.

What it means to be a ‘refugee’ in South Sudan and Uganda
After decades of armed conflict in South Sudan and Uganda, labels of ‘refugee’ and ‘internally displaced person’ fail to reflect the complex realities of the people they refer to. Leben Moro examines the history of movement across the region’s borders, and argues refugees are not the passive recipients of aid as often presented by humanitarian initiatives.
Since independence from British colonial rule, large numbers of South Sudanese and Ugandans have repeatedly crossed the shared border to escape civil wars. These forced movements of large populations have created shifting labels of ‘refugees’ and ‘internally displaced persons’ (IDPs), with tremendous social, economic and political repercussions for the persons to which these labels are applied.
In August 1955, months before Sudan’s independence, the largely Christian Southern Sudanese took up arms against Muslim rulers in the North to achieve a vision of greater regional autonomy, which sparked a mass flight of people from their homes. By the end of the First Sudanese Civil War in 1972, the Sudanese government estimated that 500,000 people had hidden in the bush, and another 180,000 had crossed into neighbouring countries, with 74,000 settling in four official camps (Onigo, Agago, Acholpii and Nakapiripirit) in northern Uganda. Many of the displaced persons, including my own family members, self-settled in other parts of Uganda, mainly near cotton ginning mills and other businesses operated by Ugandans of Indian origin, who employed them as casual labourers.
My own family members settled near Gulu, the largest town in northern Uganda, among the Acholi ethnic group. Some South Sudanese journeyed southwards to Bwelye in the centre of Uganda, where there was plentiful fertile land and jobs in Indian enterprises. Others travelled further south into the heartland of the Baganda, the largest tribe in the country, to work in sugar plantations and different enterprises, including fields where locals grew coffee, bananas and other crops.
Over time, many newcomers acquired land with their earnings and became poll taxpayers. Their receipt documentation allowed them to move across land in relative safety. In general, however, life was hard as they lacked citizenship and were vulnerable to exploitation and harassment.
The United Nations High Commissioner for Refugees (UNHCR) coordinated a programme of official repatriation, supported by public authorities in Sudan and Uganda, including a mandate that supported Sudan’s IDPs. Many people, however, chose not to leave.
In 1979, Uganda became embroiled in a bitter civil war following the overthrow of President Idi Amin Dada, forcing Southern Sudanese, including my own family members, and many Ugandans from the north of the country, to flee into the relatively peaceful Southern Sudan. The UNHCR and other humanitarian organisations as well as public authorities in Sudan helped settle many refugees in camps, but some Ugandans settled among local people, initially without external support.
The relative peace in Southern Sudan was disrupted in 1983 when the Sudan People’s Liberation Movement/Army (SPLM/A) was founded to lead another armed struggle against Sudan’s newly declared Islamic state under President Gaafar Nimeiry – which came to be known as the Second Sudanese Civil War. The violence forced Ugandan peoples living in Southern Sudan back into Uganda and many Southern Sudanese also made the crossing. Some of the refugees returned to locations they had lived in during the first civil war or joined relatives or friends who had remained in Uganda. People used their established networks.
The new wave of refugees received generous assistance from the UNHCR and the Ugandan government, whose policy was the settlement of refugees in camps and dedicated areas. Effectively, the policy redefined a refugee as ‘someone receiving assistance and living in a camp’. Many displaced Southern Sudanese avoided encampment, with its associated restrictions of movement, by self-settling among locals or dividing their family members or time between camps and outside locations.
As in the first civil war, many displaced persons in Southern Sudan did not cross international borders, but remained behind in dire circumstances. Their plight forced the United Nations to launch another initiative, Operation Lifeline Sudan, in the 1980s to assist those trapped in the war zone. This suffering formally ceased in 2005 with the conclusion of the much-lauded Comprehensive Peace Agreement between the Sudanese government and the SPLM/A, enabling the return of the IDPs to their original homes and refugees back to the country.
In 2011, Southern Sudan seceded from Sudan. About two years later, the world’s newest country relapsed into a vicious civil war. Sparked by divisions among the country’s key leaders, ethnic identities were subsequently exploited to mobilise fighters with devastating consequences for national unity and the wellbeing of civilians.
During the conflict, many Nuer people, an ethnic group primarily inhabiting South Sudan’s Nile Valley, fled into areas created on UN Mission in South Sudan (UNMISS) bases, called Protection of Civilians Sites (PoCs), to escape killing by members of the Dinka, the largest ethnic group, who had effectively taken over the country with the support of Ugandan soldiers. Nuer fighters retaliated against Dinka civilians, forcing many to flee to the Uganda border and other locations.
Many South Sudanese headed north into the new Republic of Sudan, where public authorities labelled them ’arrivals’, a new term with no precedent in refugee policy or literature, and confined them to ‘waiting stations’. Uganda also received a large number of displaced persons, among them refugees placed in settlements with international assistance. Many displaced persons settled among locals without external assistance, thus avoiding the label of ‘refugee’.
What it means to be ‘refugees’ in Uganda
The 1951 Refugee Convention states a person becomes a refugee after crossing an internationally recognised border in search of protection, recognition and status by public authorities in the asylum country or the UNHCR. When the circumstances that forced the person to seek refuge cease to exist, the refugee re-avails themselves of the country’s protection they had fled. Thus defined concrete international borders are characterised as integral to becoming a refugee or ending refuge.
For South Sudanese displaced persons, the border between their country and Uganda is not a clearly defined line separating two jurisdictions. Many parts of the border are contested by ordinary people and public authorities on both sides. Consequently, people inhabiting locations along these contested areas are not always on peaceful terms despite often belonging to the same ethnic groups, such as the Acholi of South Sudan and Uganda.
Different ethnic groups that have seen clashes over contested territories have also been forced into settling in areas of close proximity following unrest in their respective homelands. My own research reveals the Kuku of Kajokeji in South Sudan were so suspicious of the Madi in the Ugandan Moyo district that, when they settled in the latter’s region, they avoided treatment in the Moyo hospital for fear of maltreatment by Madi medical personnel. The history of conflict over certain borders has a direct bearing on the welfare of refugees in the present.
Armed groups and criminals also operate along the border, posing serious security problems, with some people losing their lives at the hands of unknown gunmen. Despite this danger, refugees and other South Sudanese cross in and out of South Sudan for matters of family and livelihoods, such as to harvest crops in their old fields due to food shortages in their new home. Others return their deceased kin to bury them decently on their old compounds and, further, trips are made to the national capital, Juba, to visit relatives or deal with administrative issues.
These movements defy the legal meaning of ‘refugee’, who is supposed to return home when the threat of persecution that caused the flight is over. They demonstrate that refugees are not the passive and docile recipients of aid, as often presented, but active individuals who exercise agency. Studies remind us that were refugees only to eat the ‘food which is distributed to them, they would die’.
What it means to stay behind as an IDP
Because IDPs are citizens living in their native county they are entitled to the same rights and legal protections as fellow citizens as stipulated by the constitution. In reality, IDPs do not always enjoy citizenship rights because those in power consider them enemies or supporters of enemies.
During the second civil war, the Sudanese government branded IDPs as rebel supporters and subjected them to all kinds of punitive measures, including starvation and denial of basic services. Many IDPs consequently starved to death or died due to deadly diseases, such as kala azar, as the already rudimentary healthcare system in pre-war Southern Sudan was destroyed by repeated military bombardments as well as frequent obstructions of international humanitarian access.
When South Sudan gained independence and descended into civil war, IDPs did not fare any better. Following shocking atrocities and the continued risk of further violence, many Nuer civilians remain in PoCs on UNMISS bases under the protection of peacekeepers in refugee-like situations. Deprived of state protection, their situation has become worse than most refugees in South Sudan, deprioritised over the dominant Dinka.
The labels of ‘refugee’ and ‘internally displaced person’ do not reflect the experiences of most South Sudanese refugees in Uganda, and IDPs within South Sudan. These terms present refugees and IDPs as powerless recipients of aid when, in reality, refugees and IDPs are active agents in efforts to improve their situation. In some cases, they creatively manipulate borders and the systems in place to satisfy their basic needs.
It has been expressed that South Sudanese refugees have shown an extraordinary creativity and resourcefulness that can form a blueprint for future refugee assistance programmes. When ‘official legal categories rarely match realities on the ground’, aid workers should now appreciate and encourage the active involvement of refugees and IDPs to address the challenges that confront them.
▻https://blogs.lse.ac.uk/africaatlse/2019/05/28/what-it-means-to-be-a-refugee-in-south-sudan-and-uganda
#réfugiés #IDPs #déplacés_internes #Soudan_du_Sud #Ouganda #histoire #histoire
U.S. is using unreliable dental exams to hold teen migrants in adult detention
The young Bangladeshi sitting in the dentist’s chair last October thought he was getting checked for diseases.
Dental staff examined his teeth, gave him a cleaning and sent him back to the juvenile facility where he had been held for months since illegally crossing the border in July.
But a checkup wasn’t the real purpose of the dental work. The government wanted to figure out if “I.J.,” as the young migrant has been identified, really was 16, as he said, or an adult.
The use of dental exams to help determine the age of migrants increased sharply in the last year, one aspect of the Trump administration’s crackdown on immigration and illegal border crossings.
The accuracy of forensic testing to help determine the age of migrants is very much a subject of the debate. And with the stakes so high, the exams are becoming another legal battleground for the government.
Federal law prohibits the government from relying exclusively on forensic testing of bones and teeth to determine age. But a review of court records shows that in at least three cases – including I.J.’s – the government did just that, causing federal judges to later order the minors released from adult detention.
In a case last year, a Guatemalan migrant was held in adult detention for nearly a year after a dental exam showed he was likely 18, until his attorneys fought to get his birth certificate, which proved he was 17.
For I.J., the results had serious ramifications. Based on the development of his teeth, the analysis showed an 87.70% probability that he had turned 18.
An immigration official reported that it was apparent to the case manager that I.J. “appeared physically older than 17 years of age,” and that he and his mother had not been able to provide a second type of identification that might prove his age.
The next month, Immigration and Customs Enforcement agents took him away in shackles and placed him in a medium-security prison that houses immigrant detainees.
He spent about five months in adult detention and 24 of those days in segregated custody. Whenever he spoke with an officer, he would say he was a minor — unaware for more than a month that his teeth had landed him there.
“I came to the United States with a big dream,” I.J. said. “My dream was finished.”
But when the Arizona-based Florence Immigrant and Refugee Rights Project took I.J.’s case to federal court, a district judge found that the Office of Refugee Resettlement’s age re-determination violated federal law and the agency’s own guidelines.
In April, the judge ordered I.J. released back into Office of Refugee Resettlement custody, a program responsible for unaccompanied migrant children. He has since reunited with his family in New York. The Florence Project also filed another case in federal court that resulted in the government voluntarily returning a Bangladeshi minor to ORR custody and rescinding his age re-determination.
As the government grappled with an influx of the number of families and children arriving at the border in fiscal year 2018, approvals of ORR age determination exams more than doubled.
These handful of cases where a minor was released from adult detention is almost certainly an undercount, as most migrants held in adult detention do not have legal representation and are unlikely to fight their cases.
It is unclear how often migrants pretend to be minors and turn out to be adults. In a call with reporters earlier this year, a Customs and Border Protection official said that from April 2018 to March 25 of this year, his agents had identified more than 3,100 individuals in family units making fraudulent claims, including those who misrepresented themselves as minors.
Unaccompanied minors are given greater protections than adults after being apprehended. The government’s standard refers migrants to adult custody if a dental exam analysis shows at least a 75% probability that they are 18 or older. But other evidence is supposed to be considered.
Dr. David Senn, the director of the Center for Education and Research in Forensics at UT Health San Antonio, has handled more than 2,000 age cases since 1998.
A program that Senn helped develop estimates the mean age of a person and the probability that he or she is at least 18. In addition to looking at dental X-rays, he has also looked at skeletal X-rays and analyzed bone development in the hand and wrist area.
He handled a larger number of cases in the early 2000s, but last year he saw his caseload triple — rising to 168. There appears to be a slowdown this calendar year for Senn, one of a few dentists the government uses for these analyses.
He said making an exact age determination is not possible.
“We can only tell you what the statistics say,” Senn said. “I think the really important thing to note is that most people who do this work are not trying to be policemen or to be Border Patrol agents or immigration …. what we’re trying to do is help. What we’re trying to do is protect children.”
In 2007 and again in 2008, the House Appropriations Committee called on the Department of Homeland Security to stop relying on forensic testing of bones and teeth. But it was the Trafficking Victims Protection Reauthorization Act of 2008 that declared age determinations should take into account “multiple forms of evidence, including the non-exclusive use of radiographs.”
In a Washington state case, an X-ray analysis by Senn showed a 92.55% probability that Bilal, a Somali migrant, already had reached 18 years of age. ICE removed him from his foster home and held him in an adult detention center.
“Not only were they trying to save themselves money, which they paid to the foster family, but they were wrecking this kid’s life,” said Matt Adams, legal director for the Northwest Immigrant Rights Project, which represented Bilal. “They were just rolling the dice.”
In 2016, a federal judge found that the Office of Refugee Resettlement relied exclusively on the dental exam and overturned the age determination for the young Somali.
Last year, in the case of an Eritrean migrant who said he was 17, Senn’s analysis of dental X-rays showed a 92.55% probability that he had turned 18, and provided a range of possible ages between 17.10 and 23.70.
It was enough to prompt his removal from a juvenile facility and placement into an adult one.
Again, a district judge found that the government had relied exclusively on the dental exam to determine his age and ordered the migrant released back into ORR custody.
Danielle Bennett, an ICE spokeswoman, said the agency “does not track” information on such reversals.
“We should never be used as the only method to determine age,” Senn said. “If those agencies are not following their own rules, they should have their feet held to the fire.”
Similar concerns over medical age assessments have sprung up in other countries, including the United Kingdom and Sweden.
The United Nations High Commissioner for Refugees’ guidance about how adolescent migrants’ ages should be analyzed says that if countries use scientific procedures to determine age, that they should allow for margins of error. Michael Bochenek, an attorney specializing in children’s rights at Human Rights Watch, said that for adolescents, the margin of error in scientific tests is “so big that it doesn’t tell you anything.”
An influx of Bangladeshi migrants claiming to be minors has contributed to the government’s recent use of dental exams. From October through March 8, more than 150 Bangladeshis who claimed to be minors and were determined to be adults were transferred from the Office of Refugee Resettlement to ICE custody, according to the agency.
In fiscal year 2018, Border Patrol apprehensions of Bangladeshi migrants went up 109% over the year before, rising to 1,203. Similarly, the number of Bangladeshi minors in ORR custody increased about 221% between fiscal 2017 and fiscal 2018, reaching 392.
Ali Riaz, a professor at Illinois State University, said Bangladeshis are leaving the country for reasons including high population density, high unemployment among the young, a deteriorating political environment and the “quest for a better life.”
In October, Myriam Hillin, an ORR federal field specialist, was told that ICE had information showing that a number of Bangladeshi migrants in their custody claiming to be underage had passports with different birth dates than on their birth certificates.
Bochenek said it’s common for migrant children to travel with fake passports that make them appear older, because in some countries minors are more likely to be intercepted or questioned by immigration agents.
While I.J. was able to regain status as a minor, three Bangladeshi migrants who crossed the U.S.-Mexico border illegally in the San Diego area in October 2018 are still trying to convince the government they are underage.
Their passports didn’t match their birth certificates. Dental exams ordered by immigration officials found that each of them had about an 89% likelihood of being adults.
“Both subjects were adamant that the passports were given to them by the ‘agent’ (smuggler), however, there is little reason to lie to any of the countries they flew into,” wrote one Border Patrol agent, describing the arrest of two of the migrants. “Also, it is extremely difficult to fake a passport, especially for no reason. I have seen [unaccompanied children] fly into each of the countries (except for Panama and Costa Rica) and pass through with no problem. This is a recent trend with Bangladeshis. They do it in order to be released from DHS custody faster.”
During interviews, the young migrants, Shahadat, Shahriar and Tareq, told asylum officers that smugglers had given them the passports, according to records from the interviews.
When asked why they had been given those birth dates, they said it had something to do with smugglers’ plans for their travel.
“I don’t have that much idea,” Shahadat told an asylum officer, according to the officer’s notes in a summary-style transcript. “When I asked why, they told me that if I don’t give this [date of birth] there will be problems with travel.”
Shahriar told the officer that the smuggler became aggressive when questioned.
The migrants have submitted copies of birth certificates, school documents and signed statements from their parents attesting to their claimed birth dates. An online database of birth records maintained by the government of Bangladesh appears to confirm their date of birth claims.
Shahriar also provided his parents’ birth certificates. If he were as old as immigration officials believe him to be, his mother would have been 12 years old when she had him.
In each case, immigration officials stood by the passport dates.
Shahadat and Shahriar are being held in Otay Mesa Detention Center. Tareq was held at the facility for months before being released on a $7,500 bond. All three are moving through the immigration system as adults, with asylum proceedings their only option to stay in the U.S..
At least one of the migrants, Shahadat, was placed in administrative segregation, a version of solitary confinement in immigration detention, when his age came into question, according to documents provided by their attorney.
A judge ordered him deported.
▻https://www.latimes.com/local/lanow/la-me-ln-immigrant-age-migrants-ice-dental-teeth-bangladesh-20190602-story.
#tests_osseux #os #âge #USA #Etats-Unis #mineurs #enfants #enfance #rétention #détention_administrative #dents #migrations #asile #réfugiés #USA #Etats-Unis

Opinion | This Is the Truth About Vaccines - The New York Times
▻https://www.nytimes.com/2019/03/06/opinion/vaccines-autism-flu.html
Vaccinations save lives, protect our children and are one of our greatest public health achievements. As public health officials, our role is to advance the health of the American people. This must include championing vaccinations.
Diseases like polio, measles, diphtheria and rubella were once common in the United States, afflicting hundreds of thousands of infants, children and adults, and killing thousands each year. Some older Americans may remember the fear associated with polio outbreaks and the era of iron lungs and leg braces — a time when swimming pools and movie theaters closed over concerns about the spread of the crippling disease. Others may recall the heartbreaking wave of rubella in the 1960s that resulted in thousands of newborn deaths, with thousands more born blind, deaf or with other lifelong disabilities.
We cannot let America be faced with these fears again. For those of us who have treated critically ill children with vaccine-preventable diseases, we know firsthand the devastation to the child — and to the family and community — of a death, limb amputation or severe brain damage that could have been avoided by a simple vaccination.
Consider measles. The World Health Organization estimates that measles vaccination prevented more than 21 million deaths worldwide since 2000. Although routine childhood vaccination for measles remains high in the United States (greater than 91 percent for preschool children), localized dips in vaccination coverage have resulted in a recent resurgence of measles in parts of the country. A total of 17 measles outbreaks affecting more than 370 individuals have been confirmed in 2018 alone, and 10 states are already reporting cases this year. Unfortunately, many more communities are at risk for outbreaks because of areas with low vaccine coverage.

How #cbd Market is moving in the right direction according to the Clinical Research and Market…
▻https://hackernoon.com/how-cbd-market-is-moving-in-the-right-direction-according-to-the-clinica
How CBD Market is moving in Right Direction According to Clinical Research and Market Analysis?Use of #cannabis to treat sick has been documented in history. The ancient healers and doctors prescribed it to their patients seeing the healing properties cannabis contained.The modern medical science only took notice of this magical family a few decades back and has been advancing to apply it in treating diseases. It is however recently the plant’s popularity picked up the pace and the market started seeing CBD or cannabis based products.CBD shouldn’t be mixed with marijuana. Though both are derived from cannabis sativa hence the term. The former does not contain enough THC (tetrahydrocannabinol) to operate as a psychoactive agent that intoxicates or causes euphoria aka the “High.” Instead, (...)
“These displaced people live in fear of being attacked at any time”
After increased insecurity in the Tillabéry region of Niger caused large numbers of people to flee their homes, MSF carried out an emergency response in early January 2019.
MSF deputy head of mission Boulama Elhadji Gori describes the situation.
Why did MSF carry out an emergency response in the rural area of #Dessa in the #Tillabéry region last week?
A state of emergency was declared recently in the department of Tillabéry, in the region of the same name. Like many other departments in the region, Tillabéry faces many security challenges.
The people living in this border area between Mali and Niger find themselves trapped in violence that comes from two directions: on one side, the community conflict; on the other, the activities of non-state armed groups.
After receiving information about people being displaced in the region, an MSF team visited the immediate area, where they saw first-hand the precarious situation in which the displaced people were living.
We are talking about a total of 1,287 people at three sites within a five-kilometre radius. These people were already vulnerable, having been displaced several times already.
What were people’s main needs?
These people had been forced to leave their homes, their fields and often their animals in order to escape the violence orchestrated by armed groups and other opportunists. Because of the hostilities in the area, basic services such as schools and health centres have been closed.
The displaced people lack shelter, food, healthcare and protection. They are also drinking untreated river water, which brings the risk of various diseases.
Given the urgency of their needs, and in the absence of other humanitarian organisations, the MSF team decided to launch a response.
What did MSF’s response involve?
Our medical team conducted 170 medical consultations, mainly for respiratory infections, malaria, dermatitis and severe malnutrition, as well as 20 antenatal consultations.
We also assessed the nutritional status of children and vaccinated nearly 130 children against measles. Five mental health promotion sessions were organised for approximately 160 people.
Several patients were referred to the health centre for follow-up care, which MSF was also involved in. Our team distributed essential relief items to 220 families, including blankets, cooking utensils, washing kits, mosquito nets and jerry cans.
To make sure that people have safe drinking water, the teams distributed 4,000 water purification tablets, and ran sessions on how to use them.
Who are the displaced people?
“Most of the people who fled the violence are women, children and the elderly, of different ethnicities, living in the border area between Mali and Niger. There are also a number of young people who reject violence and want to settle in places that are considered more secure.
The displaced include refugees from Mali and internally displaced people from Niger.
The majority of the displaced people live in fear of being attacked at any time, because of what they have already experienced – their villages being attacked, assassinations, their markets burned down, their animals stolen, and living with the threat of death.
Other than this emergency response, what is MSF doing in Tillabéry region?
MSF has been working in Niger’s Bani-Bangou department, near the border with Mali, since November 2018. Long before the state of emergency was declared, schools, health centres and other social infrastructure were not functioning because of the violence.
MSF is working in the area to ensure access to free quality medical care for displaced people and local communities. We support two health centres and five health posts.
We are also monitoring the situation in other areas which could potentially receive newly displaced people, or where there are needs not covered by other organisations, particularly in the area around Innates. MSF also supports medical services, from health posts to hospitals, in Bani-Bangou and Ouallam.
Our teams work in collaboration with the Ministry of Health. In December 2018, we treated 4,599 people, provided 452 antenatal consultations and assisted 22 births. In addition, 588 children under the age of two received routine immunisations, and 34 women of childbearing age were vaccinated against tetanus. We also referred to hospital seven patients in need of emergency treatment.
What are people’s main needs in this region? And what are the challenges of assisting them?
People in this region need food, essential relief items, physical and mental healthcare, clean water, good sanitation and hygiene, and protection.
The main challenge we face is the climate of insecurity in the region, which can make it difficult to reach the people who need assistance.
▻https://www.msf.org/displaced-people-tillabery-niger-living-fear
#IDPs #déplacés_internes #réfugiés_maliens #Mali #Niger #migrations #réfugiés

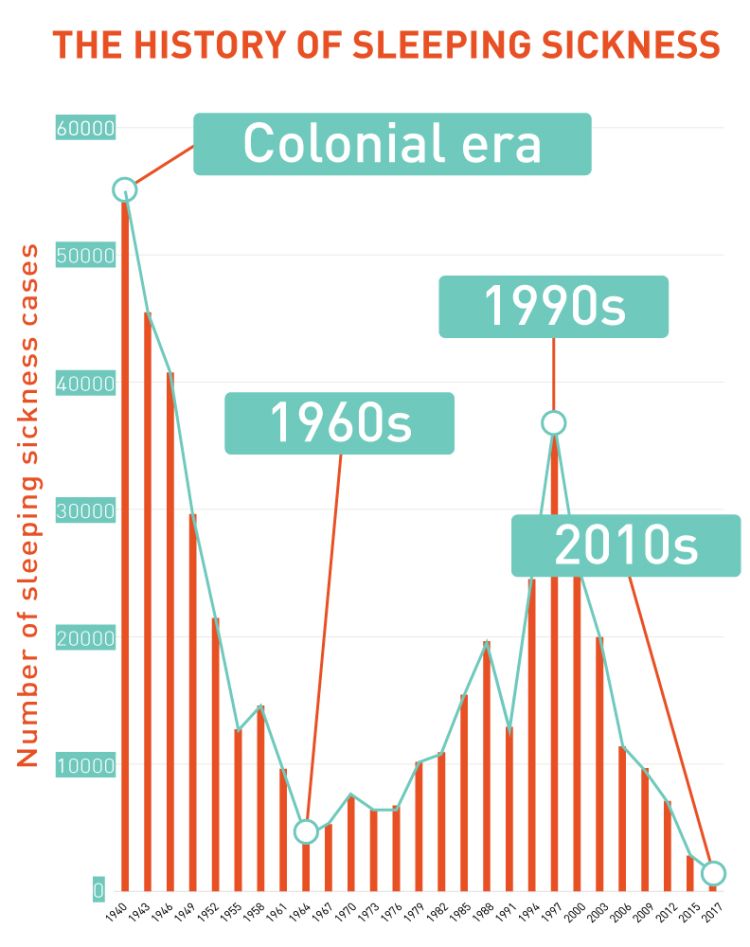
Une belle histoire pour changer : comment le DNDi a trouvé et développé un nouveau médicament contre la #maladie_du_sommeil.
Drugs for Neglected Diseases initiative (DNDi) is a collaborative, patients’ needs-driven, non-profit drug research and development (R&D) organization that is developing new treatments for neglected patients.
A doctor’s dream
▻https://stories.dndi.org/sleepingsickness-doctors-dream
#Fexinidazole, the first all-oral drug for both stages of sleeping sickness was approved in November 2018
Here are the stories of the doctors, patients, and scientists who contributed to this story
▻https://www.youtube.com/watch?v=M9tsKmK5Yms&feature=youtu.be

Un peu de #pharma quand même, puisque Sanofi est dans le coup, et doit bien y trouver son intérêt. Lors du développement d’un médicament contre la Malaria par DNDi il y a 10 ans, Sanofi en était déjà, et on pouvait lire dans Fortune :
Sanofi’s aim was not entirely altruistic, says Bernard Pécoul, executive director of DNDi, a doctor and public health specialist who spearheaded the antimalaria project. “It’s good for their image,” he says, “but it will also help with the penetration of these countries’ markets.”
Mais aussi :
[…] a nonprofit organization in Geneva, Drugs for Neglected Diseases Initiative (DNDi), had figured out a way to combine the two antimalaria drugs and was looking for a corporate partner to conduct clinical trials and market and produce the drug on a large scale. “It was the marriage of both of our needs,” says Robert Sebbag, a vice president for Sanofi.
Source : ▻http://archive.fortune.com/2008/02/22/news/international/malaria.fortune/index.htm?section=magazines_fortuneintl
Je me suis intéressé à DNDi à cette époque pour mon mémoire de master sur la question des communs immatériels dans la coopération internationale (inspiré alors du logiciel libre). Une interrogation, posée un peu vite en fin de chapitre : l’open source en matière de recherche médicale est-elle soluble dans les monopoles ?
Si des fois, le texte complet est là (en espagnol). Sur les médicaments, p22-30 :
▻http://gofile.me/2faRd/eKo0ig4JV

EMA Panel Backs First Oral-Only Drug for Deadly Disease
▻https://www.medscape.com/viewarticle/905009
Fexinidazole was developed by Sanofi-Aventis in partnership with the Drugs for Neglected Diseases initiative (DNDi), a nonprofit drug research and development organization based in Switzerland. Fexinidazole is intended exclusively for markets outside the European Union.
[...]
This is the tenth medicine recommended by the EMA under Article 58, a regulation that allows the CHMP to assess and give opinions on medicines that are intended for use in countries outside the European Union.
“The scientific opinion from the CHMP helps to support regulators in countries where regulatory capacity may be limited, by providing an expert evaluation of the medicine when used in local practice. National regulators can use the CHMP’s scientific assessment to decide on the use of the medicine in their countries,” the EMA explains.

“Is curing patients a sustainable business model?” Goldman Sachs analysts ask | Ars Technica
▻https://arstechnica.com/tech-policy/2018/04/curing-disease-not-a-sustainable-business-model-goldman-sachs-analysts-
One-shot cures for diseases are not great for business—more specifically, they’re bad for longterm profits—Goldman Sachs analysts noted in an April 10 report for biotech clients, first reported by CNBC.
The investment banks’ report, titled “The Genome Revolution,” asks clients the touchy question: “Is curing patients a sustainable business model?” The answer may be “no,” according to follow-up information provided.
Analyst Salveen Richter and colleagues laid it out:
The potential to deliver “one shot cures” is one of the most attractive aspects of gene therapy, genetically engineered cell therapy, and gene editing. However, such treatments offer a very different outlook with regard to recurring revenue versus chronic therapies... While this proposition carries tremendous value for patients and society, it could represent a challenge for genome medicine developers looking for sustained cash flow.
For a real-world example, they pointed to Gilead Sciences, which markets treatments for hepatitis C that have cure rates exceeding 90 percent. In 2015, the company’s hepatitis C treatment sales peaked at $12.5 billion. But as more people were cured and there were fewer infected individuals to spread the disease, sales began to languish. Goldman Sachs analysts estimate that the treatments will bring in less than $4 billion this year.
“[Gilead]’s rapid rise and fall of its hepatitis C franchise highlights one of the dynamics of an effective drug that permanently cures a disease, resulting in a gradual exhaustion of the prevalent pool of patients,” the analysts wrote. The report noted that diseases such as common cancers—where the “incident pool remains stable”—are less risky for business.
A game of chicken: how Indian poultry farming is creating global #superbugs
On a farm in the Rangareddy district in India, near the southern metropolis of Hyderabad, a clutch of chicks has just been delivered. Some 5,000 birds peck at one another, loitering around a warehouse which will become cramped as they grow. Outside the shed, stacks of bags contain the feed they will eat during their five-week-long lives. Some of them gulp down a yellow liquid from plastic containers - a sugar water fed to the chicks from the moment they arrive, the farm caretaker explains. “Now the supervisor will come,” she adds, “and we will have to start with whatever medicines he would ask us to give the chicks.”
The medicines are antibiotics, given to the birds to protect them against diseases or to make them gain weight faster so more can be grown each year at greater profit. One drug typically given this way is colistin. Doctors call it the “last hope” antibiotic because it is used to treat patients who are critically ill with infections which have become resistant to nearly all other drugs. The World Health Organisation has called for the use of such antibiotics, which it calls “critically important to human medicine”, to be restricted in animals and banned as growth promoters. Their continued use in farming increases the chance bacteria will develop resistance to them, leaving them useless when treating patients.
Yet thousands of tonnes of veterinary colistin was shipped to countries including Vietnam, India, South Korea and Russia in 2016, the Bureau can reveal. In India at least five animal pharmaceutical companies are openly advertising products containing colistin as growth promoters.
One of these companies, Venky’s, is also a major poultry producer. Apart from selling animal medicines and creating its own chicken meals, it also supplies meat directly and indirectly to fast food chains in India such as KFC, McDonald’s, Pizza Hut and Dominos.
▻https://www.thebureauinvestigates.com/stories/2018-01-30/a-game-of-chicken-how-indian-poultry-farming-is-creating-glob
#inde #antibiotiques #santé
Advanced #analytics and its Importance in the #healthcare Sector
▻https://hackernoon.com/advanced-analytics-and-its-importance-in-the-healthcare-sector-79603f5f9
It is understandable that anyone can feel intimidated by the huge influx of data that keeps flowing through healthcare systems every second of the day. But to draw meaningful insights from it, and use it to treat patients and prevent diseases is a big step in healthcare. This is what Big Analytics or Advanced Analytics does. The data you receive on your machines is just a jumble of ones and zeros, and you have no use for it unless you can understand what it is trying to convey.According to the survey conducted by Health Catalyst, a whopping 90% of the respondents admitted that analytics is going to be either “extremely important” or “very important” to their organization within the next few years. And the respondents also rated the importance of healthcare trends and the role played by (...)
#big-data-analytics #advanced-analytics #healthcare-analytics
#Angola : Les migrants africains en danger de mort
Les autorités angolaises lancent « la chasse aux ressortissants sub-sahariens en situation irrégulière ». Une #opération dénommée « #expatriado » est en cours en ce moment. Elle vise à « expulser tous les immigrés en situation irrégulière en Angola ». Des ressortissants maliens témoignent des « cas d’#emprisonnement suivis de pires formes de #maltraitance et d’#humiliation ». Pour l’instant, difficile d’avoir des chiffres officiels sur le nombre de Maliens victimes. Mais ceux joints sur place appellent à l’aide des autorités maliennes.
Selon certains Maliens, ces opérations d’expulsion ont débuté dans les zones minières. Elles se déroulent maintenant dans toutes les villes du pays, et concernent toutes les nationalités y compris les Maliens, qui sont parmi les plus nombreux. « Cela fait des jours que nous ne pouvons plus sortir pour aller au boulot par peur de nous faire arrêter », explique un ressortissant malien sur place. Selon lui, cette opération qui ne devrait concerner que les #sans-papiers, est aussi menée par les forces de l’ordre angolaises contre ceux qui sont en situation régulière. L’objectif, selon notre interlocuteur, est de soutirer de l’argent aux migrants.
« Une fois entre les mains des autorités angolaises, il faut payer de l’argent ou partir en prison », témoignent certains migrants maliens, avant de confirmer que plusieurs d’entre eux sont actuellement en prison. En Angola certains Maliens ont l’impression d’être « laissés pour compte par les autorités maliennes ». Pour l’Association Malienne des Expulsés, « il est inacceptable qu’un pays membre de l’Union Africaine expulse d’autres africains de la sorte ». L’AME qui juge la situation « grave » en Angola, appelle les autorités maliennes à réagir.
▻https://www.expulsesmaliens.info/Angola-Les-migrants-africains-en-danger-de-mort.html
#migrations #asile #réfugiés #rafles #expulsions #renvois #chasse_aux_migrants #migrants_maliens
Pourquoi l’Angola expulse massivement ses ressortissants congolais ?
Briefing: Problems multiply in Congo’s Kasaï
The Kasaï region in the Democratic Republic of Congo is struggling to recover from two years of intense conflict. The influx last month of more than 300,000 people from Angola, most of them long-standing migrant workers, has made a fragile humanitarian situation worse.
Here’s our briefing on the risks for the region and the new challenges for the humanitarian response.
What happened?
In attempts to clamp down on what it called illegal diamond mining operations, Angola’s government ordered the expulsion of more than 360,000 Congolese nationals, forcing them to flee in October into the Kasaï region of neighbouring DRC.
"This new shock is compounding an already dire situation in the same area that was the epicentre of the Kasaï crisis over the last couple of years,” explained Dan Schreiber, head of coordination in Congo for the UN’s emergency aid body, OCHA.
Congolese migrants and officials said the crackdown was violent, telling Reuters that dozens of people were killed, with the worst attacks occurring in Lucapa in Angola’s diamond-rich Lunda Norte province. Angolan security forces denied the allegations.
Where did they go?
Most of those expelled crossed into Kamako in Kasaï province, where aid organisations are responding to the tail-end of the Kamuina Nsapu insurgency that first erupted in 2016. Some of the returnees include refugees who fled violence in Kasaï over the last two years, the Norwegian Refugee Council said.
The NRC said conditions returnees face in Congo are “shocking”, including the risk of waterborne disease due to ineffective water and sanitation; thousands sleeping outdoors because of insufficient shelter; food prices tripling; and extortion of goods on both sides of the border.
“Hundreds of thousands of people have been robbed of their right to a dignified existence,” said Ulrika Blom, NRC’s country director in DRC. “This is not a crisis that is about to begin, it is a full-blown emergency.”
What has the reaction been?
While local communities have generally been welcoming to the returnees, OCHA’s Schreiber said skirmishes erupted in certain villages, mainly over the strain on limited food resources.
“Experience in the DRC does show that when you have a large influx of people arriving in an area it can generate tensions between host communities and the people who arrive,” he said.
Schreiber said OCHA has seen most returnees wanting to move away from the border areas and toward other destinations inland, which could help ease the humanitarian strain in Kasaï, but he also warned that more returnees could arrive from Angola.
“We don’t expect the first wave to be the last wave,” he said. “Expulsions from Angola are a cyclical phenomena that go all the way back to 2002-2003. It’s not a new phenomenon, but in this case we are seeing a major influx, and clearly the absorption capacity is not there.”
Why is their arrival in Kasaï in particular such a problem?
Kasaï was a relatively stable region in an unstable country – one currently dealing with multiple conflicts, an Ebola outbreak in North Kivu province, and one of the world’s most neglected displacement crises.
The situation in Kasaï changed dramatically in 2016 when conflict erupted between the Kamuina Nsapu anti-government movement and Congolese security forces. The inter-communal clashes spread far and wide, soon engulfing the entire region.
The conflict escalated in 2017, with massacres and mass graves, as well as general insecurity marked by banditry, and poor harvests that led to food insecurity and malnutrition.
An estimated 5,000 people have since been killed and more than 1.4 million displaced.
Toward the end of 2017 and into 2018, the crisis eased slightly, as national authorities regained control over large parts of the region. Despite isolated bouts of violence, aid groups say most militias have been formally disbanded and displaced communities are tentatively returning home.
“But those returns are accompanied by many needs, because people are returning to burned villages, destroyed homes, and a lot of destruction,” said OCHA’s Schreiber.
Two years of violence and displacement also mean locals have been unable to grow crops for three seasons, which has led to concerns over malnutrition. “We have really seen food insecurity skyrocket. So even in areas where returns have occurred, humanitarian needs have not come to an end,” Schreiber added.
What are the risks?
Although the current influx of people from Angola isn’t directly linked to the Kamuina Nsapu rebellion, aid groups are concerned about the implications of piling one problem on top of another in the same geographic area.
For the most vulnerable groups, specifically women and children, the challenges that affect those displaced by the insurgency also pose risks for the new returnees from Angola.
In May for instance, UNICEF reported that 400,000 children were “at risk of death” in the Kasaïs, because of food shortages.
Yves Willemot, a spokesman for UNICEF in Congo, said the rate of severe acute malnutrition among children living in the region has improved slightly since earlier this year but “remains challenging”.
“The security situation has clearly improved, but the impact on children is not ending in the short term,” he said.
Among those newly returned from Angola are 80,000 children. They now are also at risk, forced to walk long distances while exposed to inclement weather, hunger, and the threat of violence. Willemot said basic services are lacking for them, including access to drinking water, schooling, and treatment for diseases like malaria and measles.
Médecins Sans Frontières is among the NGOs initiating primary healthcare services for the recent arrivals, while also continuing interventions to assist the local population.
In a recent report, MSF documented alarming levels of rape in the Kasaï region, saying it treated 2,600 victims of sexual violence between May 2017 and September 2018; 80 percent of those interviewed said armed men raped them.
“The sexual violence committed in Kasaï was perpetrated largely by armed groups against non-armed people,” Philippe Kadima, MSF’s humanitarian advisor for the Great Lakes region, told IRIN. “Although the main conflict is over, we still see some violence happening in Kasaï.”
For the more than 300,000 returnees, he said there are clear humanitarian concerns, but also the risk of insecurity. “The question is, how do you keep people secure?”
“Displaced people become vulnerable, so it’s not that different to what the existing IDPs in Kasaï are going through… Security concerns, humanitarian needs, and risks of sexual violence are all factors when people become vulnerable,” he said.
What about the longer-term challenges?
Humanitarian needs remain critically underfunded in the Kasai region, said OCHA’s Shreiber, emphasising that beyond the immediate concerns are much broader needs in the region and the DRC as a whole.
He added that the humanitarian response must help minimise the long-term impact of the crisis on those affected.
“The longer we remain in this critical phase, the more we can expect to see humanitarian needs spiral out of control,” he said. “The current trigger of new humanitarian needs (the returnees from Angola) may be time-bound, but I think the impact will be lasting.”
Schreiber said the Kasaï region remains vulnerable because it faces particular challenges, including decades of underdevelopment and inaccessibility as a result of poor road infrastructure, and he urged more development actors to get involved.
“People in the Kasaïs are eager to rebound, to be back on their feet, and move on. There is no expectation that humanitarian assistance should continue forever in the Kasaï region,” he said. “People want to be autonomous, but what they need is support to build up their resilience and be able to move towards a situation where their most basic needs are met and they are able to think about their futures again.”
Les violations des droits humains des migrants africains en Angola
Les violations des droits humains des migrants africains en Angola
Depuis un certain moment, la communauté africaine vivant sur le territoire angolais est l’objet de toute sorte de violation de ses droits les plus fondamentaux par les autorités de ce pays. La Charte Africaines des Droits de l’Homme et des Peuples protège les droits des migrants dans tous ses aspects contre les violations des droits et l’Angola est justement membre de l’Union Africaine. Ainsi, ces violations se matérialisent par des arrestations musclées et arbitraires, des emprisonnements dans des conditions inhumaines et dégradantes (art.5 de la Déclaration Universelle des Droits de l’Homme et de la Charte Africaine des Droits de l’Homme et des Peuples) de même que les expulsions collectives pourtant interdites par la Charte Africaine dans son article 12.5.
L’AME est vivement préoccupée par les récentes arrestations, détentions et expulsions des centaines de milliers de migrants africains dont des maliens. Selon des informations recueillies auprès de nos sources sur place, une centaine de maliens sont concernés par cette situation qui évolue et change de jour en jour.
Nous attirons l’attention de l’Union Africaine et de ses pays membres sur la situation inacceptable que vivent les étrangers sur la terre africaine d’Angola et rappeler que les droits de l’homme sont des droits inaliénables de tous les êtres humains, quels que soient leur nationalité, leur lieu de résidence, leur sexe, leur origine ethnique ou nationale, leur couleur, leur religion…
L’Angola comme la plupart des pays africains s’est engagé à protéger, respecter et réaliser les droits de l’homme, non seulement de ses nationaux, mais de toute personne sous sa juridiction. Dans ce contexte, tous les étrangers se trouvant sur le sol angolais auraient dû bénéficier de la protection des autorités angolaises quelque soient les raisons qu’elles mettent en avant pour justifier ces expulsions.
L’Organisation des Nations Unies (ONU) n’est pas resté silencieuse comme la plupart des pays africains, le Haut-Commissaire des Nations Unies aux droits de l’homme a mis en garde sur les conséquences des expulsions massives de réfugiés depuis l’Angola, au cours des trois dernières semaines de ce mois d’octobre.
Par ailleurs, le Secrétaire Général des Nations Unies a rappelé le 19 septembre 2017 que : « tout pays a le droit de contrôler ses frontières. Mais cela doit se faire de telle sorte que les droits des personnes ‘en mouvement’ soient protégés ».
Au regard de tout ce qui vient d’être évoqué :
1. L’Association Malienne des Expulsés (AME) pour sa part, exhorte le gouvernement Malien à tout mettre en œuvre pour la sécurisation de nos compatriotes et de leurs biens dans les pays d’accueil ;
2. Appelle le gouvernement à communiquer davantage sur cette situation en donnant beaucoup plus d’informations aux familles des maliens vivants en Angola ;
3. Encourage le gouvernement de continuer à œuvrer pour le respect des droits des migrants maliens et aussi pour le développement d’une relation franche entre les Etats africains en vue de la réalisation de l’unité africaine comme le prévoit l’article 117 de la Constitution ;
4. Invite l’Union Africaine à dénoncer et prendre des mesures contre les violations des droits humains dans les pays membres ;
5. Invite également les Etats membres de l’Union Africaine à renoncer aux expulsions massives des ressortissants d’autres pays africains et à mettre fin sans délais aux opérations actuelles en cour ;
6. Exhorte l’U.A et les Etats à une plus grande implication des organisations de la société civile aux différents processus pour la gestion de la migration.
▻http://www.expulsesmaliens.info/Les-violations-des-droits-humains-des-migrants-africains-en-Angola
Opinion | We Know How to Conquer Tuberculosis - The New York Times
▻https://www.nytimes.com/2018/09/26/opinion/we-know-how-to-conquer-tuberculosis.html
And so, tuberculosis remains the world’s leading infectious disease killer, by far. It infects some 10 million people around the world every year, killing roughly 1.5 million. That’s some 4,000 deaths per day. By comparison, Ebola killed four people in 2017. America’s opioid epidemic kills about 115 people a day.
Still, tuberculosis is rarely the stuff of headlines. It’s ancient. It normally affects only the poorest people in the poorest countries. And when it does spread through wealthier areas, it’s generally curable with antibiotics. But a contingent of doctors, scientists and public health officials have spent the past two decades battling a global epidemic of the disease. And on Wednesday, they got their first hearing at the United Nations General Assembly. In a high-level meeting exclusively about tuberculosis control, those experts called on world leaders to devote more attention and far more resources to the disease. Both are urgently needed. Tuberculosis receives significantly less funding than H.I.V. or malaria, even though TB kills more people each year than both of those diseases combined. The World Health Organization estimates a $3.5 billion funding shortfall for TB control efforts, and says that gap could double in five years.
But policymakers, industry leaders and doctors on the front lines might also consider a change in strategy: Treat tuberculosis outbreaks in poor countries the same way they are treated in rich ones. That is, don’t just treat those who are sick; find and test their household members, neighbors, classmates and colleagues — and then treat the ones who test positive. Give them medications to kill the bacteria before they develop symptoms and before they pass the bacteria on, through their own coughing, to the next victim.
United States Patent : 9861628
▻http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO1&Sect2=HITOFF&d=PALL&p=1&u=%2Fnetahtml%2FPTO%2Fsrchnum.htm&r=1&f=G&l=50&s1=98,61,628.PN.&OS=PN/98,61,628&RS=PN/98,61,628
Buprenorphine-wafer for drug substitution therapy
Abstract
The present invention relates to oral pharmaceutical dosage forms comprising buprenorphine with the dosage form releasing buprenorphine instantly upon oral, preferably sublingual, application of the dosage form. The present invention also relates to the use of such dosage forms for treating pain in a human or animal or for drug substitution therapy in drug-dependent human subjects.
BACKGROUND OF THE INVENTION
Chronic pain, which may be due to idiopathic reasons, cancer or other diseases such as rheumatism and arthritis, is typically treated with strong opioids.
Over the last decades prejudices in the medical community as to the use of strong opioids for treating chronic pain in patients has significantly decreased. Many of the se prejudices were due to some of the characteristics being inherent to opioids.
While opioids have always been known to be useful in pain treatment, they also display an addictive potential in view of their euphorigenic activity. Thus, if opioids are taken by healthy human subjects with a drug seeking behaviour they may lead to psychological as well as physical dependence.
These usually undesired characteristics of opioids can however become important in certain scenarios such as drug substitution therapies for drug addicts. One of the fundamental problems of illicit drug abuse by drug addicts ("junkies") who are dependent on the constant intake of illegal drugs such as heroin is the drug-related criminal activities resorted to by such addicts in order to raise enough money to fund their addiction. The constant pressures upon addicts to procure money for buying drugs and the concomitant criminal activities have been increasingly recognised as a major factor that counteracts efficient and long-lasting withdrawal and abstinence from drugs.
Therefore, programmes have been developed, particularly in the United States and western European countries, in which drug addicts are allowed to take prescription drugs under close supervision of medical practitioners instead of illegal drugs such as street heroin.
The aim of drug substitution theory is thus to first enable addicts to lead a regular life by administering legal drugs to prevent withdrawal symptoms, but because of their legal character and prescription by medical practitioners do not lead to the aforementioned described drug-related criminal activities. In a second and/or alternate step in the treatment of drug addiction may be to slowly make the drug addict less dependent on the drug by gradually reducing the dose of the substitution drug or to bridge the time until a therapy place in a withdrawal programme is available.
The standard drug used in drug substitution therapy programmes has for a long time been methadone. However, in recent years the potential of other opioids as substitution drugs in substitution therapy has been recognised. A particularly suitable drug for that purpose is the opioid buprenorphine, which is a mixed opioid agonist/antagonist.
Nowadays, buprenorphine preparations are administered in drug substitution programmes in the form of a tablet for sublingual administration. One of the reasons that the tablets are formulated for sublingual administration is that this the preferred route of administration for buprenorphine. Furthermore, if a patient swallows such tablets they will not provide euphorigenic activity.
One example of sublingual tablets for drug substitution therapy is the preparation Subutex.RTM. (being marketed in Germany by Essex Pharma).
Nevertheless, drug addicts sometimes still try to divert these sublingual buprenorphine tablets by removing them from the mouth when the supervising healthcare professional’s attention is directed to other activities. Later the tablets may be sold or the active agent buprenorphine isolated/extracted to apply it parenterally.
Another buprenorphine preparation aimed at preventing this potential possibility of abuse has recently gained administrative approval in the United States (Suboxone.RTM.). The Suboxone.RTM. preparation comprises buprenorphine hydrochloride and the opioid antagonist naloxone hydrochloride dihydrate. The presence of naloxone is intended to prevent parenteral abuse of buprenorphine as parenteral co-administration of buprenorphine and naloxone in e.g. an opioid-dependent addict will lead to serious withdrawal symptoms.
However, there remains a need for other diversion and/or abuse-resistant dosage forms of buprenorphine, which can be used in drug substitution therapy as described above. Additionally, it would be desirable to have a buprenorphine preparation available which is diversion and/or abuse-resistant in cases where the preparation is used for drug substitution therapy and which could also provide efficient analgesia in cases where the preparation is administered to alleviate pain in a patient.
OBJECT AND SUMMARY OF THE INVENTION
It is an object of the present invention to provide an oral pharmaceutical dosage form of the active agent buprenorphine that is less prone to diversion and/or abuse in drug substitution therapy. It is another object of the present invention to provide an oral dosage form of the active agent buprenorphine that can be used for drug substitution therapy and/or pain treatment.
In one embodiment the present invention relates to an oral pharmaceutical dosage form comprising at least buprenorphine or a pharmaceutically acceptable salt thereof with a dosage form releasing buprenorphine or said pharmaceutically acceptable salt thereof instantly upon or oral, preferably sublingual, application of the dosage form. It is, however, understood that the invention and its various embodiments which are set out below, can be extended to any opioid or analgesic whose preferred route of administration is oral, prefereably sublingual, as is the case for buprenorphine.
An instant release of buprenorphine or a pharmaceutically acceptable salt thereof upon oral, preferably sublingual, application means that substantially all of the buprenorphine or said pharmaceutically acceptable salt thereof will be released within less than three minutes, preferably within less than two minutes or less than one minute. Even more preferably, substantially all of the buprenorphine or said pharmaceutically acceptable salt thereof will be released within less than thirty seconds, twenty seconds, ten seconds or even within less than five seconds after oral, preferably sublingual, application of the dosage form. In one of the preferred embodiments these oral dosage forms will comprise between approximately 0.1 mg and approximately 16 mg buprenorphine or the equivalent amounts of a pharmaceutically acceptable salt thereof.
In a further preferred embodiment these oral pharmaceutical dosage forms will achieve an average C.sub.max of between 1.5 ng/ml and approximately 2.25 ng/ml in the case of a dose of 0.4 mg buprenorphine hydrochloride being administered. In the case of a dose of 8 mg buprenorphine HCl being administered, the C.sub.max will typically be between approximately 2.5 and 3.5 ng/ml and if a dose of 16 mg buprenorphine hydrochloride is administered the C.sub.max will preferably be between 5.5 to 6.5 ng/ml.
Yet another preferred embodiment of the invention relates to oral pharmaceutical dosage forms which may provide for the above-mentioned characteristics and/or an average Tmax of from approximately 45 to approximately 90 minutes.
In a particularly preferred embodiment the dosage forms will additionally comprise an opioid antagonist, preferably naloxone or a pharmaceutically acceptable salt thereof.
In yet a further preferred embodiment, the pharmaceutical dosage form will comprise buprenorphine and the opioid antagonist, which preferably is naloxone, in a weight ratio of from approximately 1:1 to approximately 10:1.
One embodiment of the present invention also relates to oral pharmaceutical dosage forms, which may have some or all of the aforementioned characteristics and wherein the dosage form has a film-like or wafer-like shape.
Another embodiment relates to a method of manufacturing the afore-mentioned described dosage forms.
Embodiments of the present invention also relate to the use of the afore-described oral, preferably sublingual, pharmaceutical dosage forms in the manufacture of a medicament for treating pain in a human or animal and/or for drug substitution therapy in drug-dependent human subjects.
One aspect of the invention also relates to a method of drug substitution therapy in drug-dependent human subjects wherein the aforementioned oral pharmaceutical dosage forms are administered to a drug-dependent subject in need thereof.
Haven’t heard of RNA therapy yet? You will
▻https://massivesci.com/articles/rna-therapy-treatments
After a decade of painstaking progress, the underdog is on the brink of treating a broad range of diseases
We still don’t know all the consequences of gene manipulation
▻https://massivesci.com/articles/frankenstein-edraki
Genome meddling to cure diseases is often worth the risk, but nothing else is just yet
Back pain: how to live with one of the world’s biggest health problems | Society | The Guardian
▻https://www.theguardian.com/society/2018/jun/14/back-pain-how-to-live-with-one-of-the-worlds-biggest-health-problems
This month, the Lancet published a series of three papers written by a large, international group of experts who came together to raise awareness of the extent of the problem of low back pain and the evidence for recommended treatments. The authors were scathing about the widespread use of “inappropriate tests” and “unnecessary, ineffective and harmful treatments”.
The papers tell us low back pain is an “extremely common symptom, experienced by people of all ages”, although it peaks in mid-life and is more common in women than in men. There are 540 million people affected globally at any one time and it is the main cause of disability worldwide.
The six-year investigation that began as an attempt to find relief from her own pain and ended up exposing an exploitative, corrupt and evidence-free $100bn industry, is fittingly described in the title of her book: Crooked.
The camera lies … MRI scans show up disc degeneration but unfortunately most people will have some. Photograph: HadelProductions/Getty Images
The proliferation of unnecessary and risky interventions has been far worse in the US, with its insurance-based healthcare system, than in the NHS. But the UK is far from immune. When a healthcare system functions as a marketplace, there will inevitably be incentives for certain treatments to be pursued over others, for services that can generate a surplus. It is a struggle for patients and clinicians everywhere to resist pain medication that is incredibly effective in the short term, even if it is incredibly harmful in the long term.
“Nearly everybody gets back pain at some point in their life,” says Martin Underwood, co-author of the Lancet series, a GP and a professor at Warwick Medical School. “For most people, it’s a short-term episode that will resolve over a period of days or weeks, without the need for any specific treatment. They catch or twist or stretch something, and it’s awful, and then it gets better.” Of those who experience a new episode of back pain, under 1% will have serious causes that need specific treatment for issues such as cancer in the spine, a fracture, diseases or infection, he says. But there is another group, in which, “after the natural period of healing – normally six weeks for most things – people go on to get pain lasting months and years, which can be very disabling, even though the original cause of the pain is no longer there. We would label this as nonspecific low back pain, simply because we don’t know what is causing the pain.”
“At best, these spine surgeons define success as a 38% improvement in pain and function,” says Ramin, “but if a hip or a knee surgeon had a 38% success rate, that physician would no longer do that surgery. And 38%? I think that’s really optimistic.” In her book, she describes the scandal of the Pacific Hospital in Long Beach, California, which carried out more than 5,000 spinal fusion surgeries. “Surgeries were being performed on large numbers of patients who were often immigrants – Spanish-speaking labourers – and being billed to workers’ compensation insurance or public health insurance. Could you do worse than butcher these Latino field workers who don’t understand what’s happening to them, but are being told they can get free medical care?”
We like to think that this could never happen in the UK, and Underwood admits there is a huge difference between the two healthcare systems. “Most spinal surgeons in the UK will avoid operating for nonspecific low back pain because they’re aware of all these problems,” he says. “But there is still pressure from patients for something to make them better, and some people are still getting operated on. My advice for anybody is: don’t have surgery for back pain unless there is a clear, specific indication.”
When I ask Underwood what works, he tells me: “Whatever you do for a patient at a time when their back is really bad, the chances are they’re going to be a lot better three weeks later. So we treat people and we see them getting better and we ascribe their improvement to the treatment we’ve given, but we know that natural improvement over time is always much larger than the positive effect you get from the treatment.” The evidence is strongest for therapist-delivered interventions such as the cognitive behavioural approach, based on the same principles as CBT, exercise treatment and physiotherapy. He has also worked on a trial that showed training physiotherapists to deliver the cognitive behavioural approach in a group, combining movement and reassurance about movement, is helpful to patients and could be delivered in the NHS at low cost.

Goldman Sachs report : « Is curing patients a sustainable business model ? » / Boing Boing
▻https://boingboing.net/2018/04/14/shared-microbial-destiny.html
Soigner les pauvres est seulement rentable s’ils demeurent malades.
In Goldman Sachs’s April 10 report, “The Genome Revolution,” its analysts ponder the rise of biotech companies who believe they will develop “one-shot” cures for chronic illnesses; in a moment of rare public frankness, the report’s authors ask, “Is curing patients a sustainable business model?”
The authors were apparently spooked by the tale of Gilead Sciences, who developed a Hepatitis C therapy that is more than 90% effective, making $12.5B in 2015 — the year of the therapy’s release — a number that fell to $4B this year.
The analysts are making a commonsense observation: capitalism is incompatible with human flourishing. Markets will not, on their own, fund profoundly effective cures for diseases that destroy our lives and families. This is a very strong argument for heavily taxing the profits of pharma companies’ investors and other one percenters, and then turning the money over to publicly funded scientific research that eschews all patents, and which is made available for free under the terms of the Access To Medicines treaty, whereby any country that devotes a set fraction of its GDP to pharma research gets free access to the fruits of all the other national signatories.
Humans have shared microbial destiny. If there’s one thing that challenges the extreme libertarian conception of owing nothing to your neighbor save the equilibrium established by your mutual selfishness, it’s epidemiology. Your right to swing your fist ends where it connects with my nose; your right to create or sustain reservoirs of pathogens that will likely kill some or all of your neighbors is likewise subject to their willingness to tolerate your recklessness.
Goldman Sachs’s analysts suggest three “cures” for the problem of one-shot cures; and taxing the rich to fund socialized pharma research isn’t among them; rather, they propose eschewing rare diseases, to ensure that the pool of patients is large enough to produce a return on their investment, or developing one-shot cures fast enough to “offset the declining revenue trajectory of prior assets.”

Charting Death
▻https://owenshen24.github.io/charting-death
Well, it turns out there’s a fascinating study conducted by Paul Slovic and Barbara Combs where they looked at how often different types of deaths were mentioned in the news. They then compared the frequency of news coverage with the actual frequency of people who died for each cause.
The results are what one might cynically expect:
“Although all diseases claim almost 1,OOO times as many lives as do homicides, there were about three times as many articles about homicides than about all diseases. Furthermore, homicide articles tended to be more than twice as long as articles reporting deaths from diseases and accidents.”
Since 1979, when the original Combs and Slovic study was conducted, there have been several more empirical analyses which have found largely similar results. (Notably, here and here)
Scientists are trying to cure diseases by harnessing our own cells
▻https://massivesci.com/articles/rett-syndrome-drug-combination-treatment
New research on Rett syndrome, caused by a mutated gene, suggests a treatment to reverse some disease symptoms
Those 2-Minute Walk Breaks? They Add Up - The New York Times
▻https://www.nytimes.com/2018/03/28/well/move/walking-exercise-minutes-death-longevity.html
Walk for two minutes. Repeat 15 times. Or walk for 10 minutes, thrice. The benefits for longevity appear to be almost exactly the same, according to an inspiring new study of physical activity patterns and life spans.
It finds that exercise does not have to be prolonged in order to be beneficial. It just has to be frequent.
Most of us who are interested in health know that federal exercise guidelines recommend we work out moderately for at least 30 minutes per day at least five times per week in order to reduce our risks of developing many diseases or dying prematurely.
These guidelines also recommend that we accumulate those 30 minutes of daily exercise in bouts lasting for at least 10 minutes at a time.
The guidelines, first published in 2008, were based on the best exercise science available at the time, including several studies indicating that if exercise sessions were briefer than 10 minutes, they would not increase people’s aerobic fitness, meaning their athletic endurance.
But improving endurance is not the same thing as improving health.
Sixth edition of The Tobacco Atlas launched today
The sixth edition of The Tobacco Atlas was launched today at the 17th World Conference on Tobacco or Health in Cape Town, South Africa. The publication shows that the tobacco industry is increasingly targeting vulnerable populations in emerging markets, such as Africa, Asia, and the Middle East, where people are not protected by strong tobacco control regulations.
The Atlas, which is co-authored by American Cancer Society (ACS) and Vital Strategies, shows the scale of the tobacco epidemic around the globe. It highlights where progress has been made in tobacco control, and describes the latest products and tactics being deployed by the tobacco industry to grow its profits and delay or derail tobacco control efforts. In response to an evolving tobacco control landscape, the Sixth Edition includes new chapters on regulating novel products, partnerships, tobacco industry tactics and countering the industry.
“The Atlas shows that progress is possible in every region of the world. African countries in particular are at a critical point – both because they are targets of the industry but also because many have opportunity to strengthen policies and act before smoking is at epidemic levels.” said Jeffrey Drope, PhD, co-editor and author of The Atlas and Vice President, Economic and Health Policy Research at the American Cancer Society.
At the press conference where The Atlas was launched, Emma Wanyoni from Kenya Tobacco Control Alliance and the Kenya International Institute of Legislative Affairs, spoke about the challenges they have face in Kenya, where it took 10 years to get a tobacco control policy put in place, she urged governments to act now with tough tobacco control laws to avoid the unnecessary injuries and death caused by tobacco.
“The Atlas shows that wherever tobacco control is implemented, it works. People benefit economically and in improved health. And the industry rightly suffers,” said José Luis Castro, President and Chief Executive Officer of Vital Strategies.
“Tobacco causes harm at every stage of its life cycle, from cultivation to disposal,” said Dr. Neil Schluger, Vital Strategies’ Senior Advisor for Science and co-editor and author of The Atlas. “It is linked to an ever-increasing list of diseases, burdens health systems, and exacerbates poverty. The only way to avert this harm is for all governments to vigorously implement the Framework Convention on Tobacco Control and to enforce the proven strategies that reduce tobacco use.”
Dr Schluger stressed that while Africa has seen real successes in tobacco control recently, economic growth has increased consumers’ ability to afford tobacco products and there is a lack of tobacco control interventions to deter tobacco use. The Sixth Edition of The Tobacco Atlas reveals that the tobacco industry deliberately targets countries that lack tobacco control laws and exploits governments, farmers and vulnerable populations across Africa.

The Quiet Revolution of CRISPR - Facts So Romantic
▻http://nautil.us/blog/the-quiet-revolution-of-crispr
CRISPR’s not on the cusp of anything.WikicommonsHow many diseases could humans treat if the DNA in troublesome cells could be edited within the body? Half? Most? How about “absolutely everything”? That was the answer Irina Conboy, a bioengineer at U.C. Berkeley, recently gave to New Scientist. Her optimism illustrates the promise, announced three years ago, of CRISPR-Cas9—the new tool scientists have to edit the genome directly, quickly, and cheaply.What progress might 2018 bring? In October the website Futurism declared, “CRISPR Is on the Cusp of Eradicating a Host of Diseases.” It’d be more accurate to say CRISPR is close to starting some clinical trials on eradication. “The field is currently over-optimistic about possible results of clinical trials,” Alexey Bersenev, the director of the (...)
‘It’s a Slow Death’: The World’s Worst Humanitarian Crisis - The New York Times
►https://www.nytimes.com/interactive/2017/08/23/world/middleeast/yemen-cholera-humanitarian-crisis.html
SANA, Yemen – After two and a half years of war, little is functioning in Yemen.
Repeated bombings have crippled bridges, hospitals and factories. Many doctors and civil servants have gone unpaid for more than a year. Malnutrition and poor sanitation have made the Middle Eastern country vulnerable to diseases that most of the world has confined to the history books.
The rise and fall and rise again of 23andMe : Nature News & Comment
►http://www.nature.com/news/the-rise-and-fall-and-rise-again-of-23andme-1.22801
23andme has always been the most visible face of direct-to-consumer genetic testing, and it is more formidable now than ever before. In September, the company announced that it had raised US$250 million: more than the total amount of capital raised by the company since its inception. Investors estimate that it is worth more than $1 billion, making it a ’unicorn’ in Silicon Valley parlance — a rare and valuable thing to behold. But for scientists, 23andme’s real worth is in its data. With more than 2 million customers, the company hosts by far the largest collection of gene-linked health data anywhere. It has racked up 80 publications, signed more than 20 partnerships with pharmaceutical firms and started a therapeutics division of its own.
“They have quietly become the largest genetic study the world has ever known,” says cardiologist Euan Ashley at Stanford University, California.
Scientists, meanwhile, were dubious. Family history was and is still a more powerful indicator than genes are for predicting the risk of most diseases. “The evidence is increasingly strong that the benefits of direct-to-consumer testing for these kinds of indications are somewhere between small and zero,” says Stanford University lawyer and ethicist Hank Greely, a long-time critic of the company.